Loading 
Bonanza Offer FLAT 20% off & $20 sign up bonus Order Now
Question:
According to the article by Asif, Jas, Irwin & Manit (2014) a clinical review of erectile dysfunction in men, erectile dysfunction in males is defined as diminished ability of an individual to successfully achieve and maintain a penile erection in nature that can bring about satisfactory sexual intercourse with their partner. It is crucial to comprehend the causes, risk factors, assessment and recognition of this condition in an effort to develop and provide appropriate and effective management strategies. According to the research reports provided by Massachusetts male aging study survey on males aged between 40-70 years, it was found that more than 50% of the men involved in the survey have had an erectile dysfunction at least once in their sexually active life. This condition is non-specific to cultural background or age. However, it is noted in the article that erectile dysfunction prevalence increases with advancement of age. The condition has a significant impact on the physical, mental, emotional and psychological wellbeing of an individual. Most importantly, it results in reduced confidence in most of the affected persons and hence affecting their sexual relationship with others. Most of the concerned people never seek any medical attention, but the situation is slowly improving as there is an improvement in public awareness and universal availability of effective medical management.
The article stipulates that there are various causes of this condition that include psychogenic causes that are attributed to stress, anxiety, psychological disorders, mental illness and medication prescribed for the treatment of these diseases and organic causes that affect the neurovascular and biochemical pathways. Notably, in most patients both causes contribute to the development of the condition. Other chronic diseases that are implicated in the establishment of erectile dysfunction include hypertension, diabetes, and obesity (Thorve et al. 2012). The lifestyle risk factors that are associated with it are cigarette smoking which is also one of the leading causes of the development of atherosclerosis, bicycle riding especially for mild to moderate dysfunction and sedentary lifestyle. As well the particular medications that contribute to the causation of the condition are antidepressants, antihypertensive, cardiac drugs, diuretic drugs, hormonal drugs, histamine receptor 2 antagonist and recreational substances such as alcohol and cocaine among others.
Assessment of men with predisposing health conditions to erectile dysfunction especially those having diabetes, hypertension, and urinary tract infections should be done regularly as part of primary health care. As stated by Perelman, (2011), this will ensure early detection and identification of the dysfunction and manage it with drugs having the lowest acquisition cost. Equally, medical and sexual histories can be combined with other investigations during the primary care provision. Identification of risk factors and predisposing factors trigger provision of health education and early treatment before further deterioration of the condition.
For a health care provider to differentiate between psychogenic and organic caused erectile dysfunction, a medical provider should gather adequate and comprehensive history from the client in order to determine the onset of the condition and the factors that triggered its onset. Psychogenic related erectile dysfunction is significantly higher among young males as compared to the elderly with no risk factors that can be readily identified, and it can be associated with sexual relationship challenges. Another defining characteristic is that the erection is sustained during masturbation or when having sex with another partner. Clinical examination is an essential part of the diagnosis as it helps note any abnormalities in the anatomy and physiological functioning of the genitalia and various related organs such as the prostate glands. In addition, vital signs and body mass index recording as part of the assessment process can help in diagnosing other underlying conditions that can possibly contribute to worsening of the dysfunction.
Primary care treatment options available are lifestyle modifications that range from performing physical exercises, stopping alcohol intake, smoking, and weight loss. These strategies not only do they prevent or make one recover from the erectile dysfunction but also reduces one’s risk of developing cardiovascular conditions and type 2 diabetes. There are also suggested herbal treatments as well and conventional therapies. However, most clinicians don’t recommend herbal remedies due to lack of evidence from clinical studies concerning them. Conventional drugs that are available for treatment are oral phosphodiesterase inhibitors such as sildenafil considered as the first line that can be offered in the initial stages of the condition by primary health care providers. This medication is contraindicated for patients having hypotension, cardiac diseases, consuming nitrates, renal and hepatic impairments. Another option utilized by the secondary management team is injectable prostaglandins that are administered into the intracavernosal and transurethral sites. Moreover, before the initiation of these therapies health education is offered to the clients with regard to the side effects risk factors and adherence to the dosage of the prescribed drugs.
As stipulated in the article by Francis & Corbin (2011), earlier studies involving 112 individuals with erectile dysfunction divided into two groups using sildenafil and a placebo for 24 weeks, sildenafil shows 69% effectiveness in curbing the condition as compared with 22% among those who used a placebo. Another available advanced option in the management is the use of vacuum erection devices. However, it may be accompanied by complications such as pain, bruising, and necrosis. It ensures high patient and partner satisfaction rates of between above 82% and 84% respectively. Finally, the third and last treatment alternative are surgery and fitting with a prosthesis if the dysfunction is nonresponsive to drugs and other therapies. The two types of prosthesis are malleable and inflatable ones. The satisfaction rates are high even though there are some malfunctioning that can be anticipated in some cases (Glina, 2011).
In conclusion, sexual dysfunction is one of the pertinent health issues in reproductive health. Men of all age groups are mostly affected by erectile dysfunction. Primary health care, as well as proper reproductive health education, should be provided to individuals in order to reduce its occurrence and prevalence by avoiding causative factors and risk factors. Primary care, early diagnosis, and management are both cheaper and efficient. In my opinion, partners should be encouraged to be supportive of each other in order to curb psychogenic related dysfunction besides seeking medical attention together.
Conception entails timing of oneself. One should ensure conditions are favorable for the ovum and sperm cells to come into contact with one another and fertilization to occur.The menstrual cycle can be utilized and relied upon to give one signs on when the cycle is almost beginning and what is expected at different stages within the entire period of the menstrual cycle. The first step to ensuring anticipatory conception is to learn the days when one is optimally fertile. According to McKerns and Kenneth (2012), most women have a 28-day menstrual cycle. This means one has about 6 days each month when there are high chances of conceiving. This includes the day one of your ovaries releases an ovum in a process referred to as ovulation and 5 days following the ovulation when the ovum is still viable. Having sex within that window is key in predisposing one to conception.
Within the the first and initial half of the menstrtal and ovarian cycle estrogen hormone levels increase significantly. Estrogen makes the lining of the muscles of the uterus proliferate and thicken. On the forteenth day of an average twenty eight day cycle, the ovum released during ovulation moves from the ovary towards the uterus through the oviduct. Estrogen hormone levels rise throughout the body and are implicated in the preparation of the uterus surface ready for conception and implantation. One has high chances of conceiving on the tird day prior to or on ovulation day. However, some individuals with irregular cycles may ovulate earlier or later than day 14.
Conception occurs when the ovum is fertilized the sperm cell after which it is implanted on the fundus are of the uterine wall. If the ovum does not get fertilized, it will break unevenly, and fertilization will not take place (Kenneth, 2012). Few years after inception of menstrual cycle , irregular cycles are commonly experienced. Usually, the cycle takes between 21 to 35 days. For practical figuring of one's cycle , charting of the menstrual cycle and recording of its duration is important. Since the length of the cycle can vary from one month to another, it is essential for one to keep a record of each cycle. From the records, one can obtain the mean value of the days each cycle takes after which 18 days are subtracted from the duration of the shortest cycle. This is the possible day one be fertile hence conceive. Alternatively, 11 days can be subtracted from the length of the longest cycle. This is the last day one is also likely to be fertile, and sexual intercourse is encouraged during these fertile days for couples aiming to have a baby (Runnebaum, 2012).
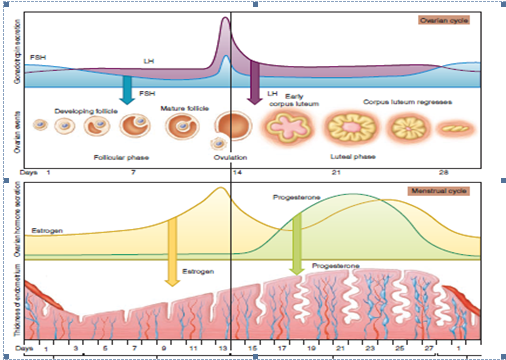
Fig.1. Stages of the ovarian cycle
Various stages are triggered by physiological changes throughout the cycle in phases. On the first day of the cycle, the uterine endometrium starts to shed off as menstrual bleeding from the vagina which usually about four to six days. The ssubsequent phase, the follicular phase a the follicle becomes ready for release from the ovary. Under normal circumstances, only one ovum is released in each cycle. This process differs with others who have short or extended periods. The last three days of the follicular phase including ovulation day, are your fertile days. This is the time when one is most likely to become pregnant if they have sex without using contraception (Foster & Wynn, 2012).
The third phase, luteal phase, is a period that starts during the day of ovulation when the ovum is released from the egg follicle . It happens anytime from Day 7 to Day 22 of a menstrual cycle. If the ovum gets fertilized by deposited a sperm and implants to the endometrium, pregnancy results. Unsuccessful fertilization or implantation leads to the endometrium breaking down.
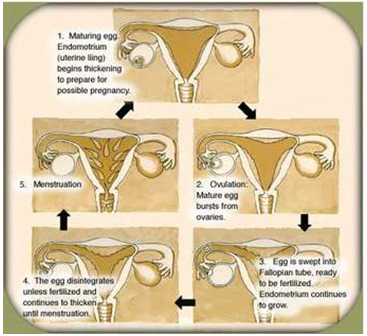
Fig.2. ovarian and menstrual cycles
Fertility window can be determined by use of the body’s physiological changes such as temperature changes that are noted after ovulation. One can accurately monitor their basal temperatures by use of a clinical thermometer which is regarded to be more sensitive than standard ones and will show temperature changes down to a significant fraction of a degree. Measuring of temperatures are is recommended at a specified time each morning, immediately after getting out of bed before performing any activities in order to get accurate readings (Guillebaud, 2012).
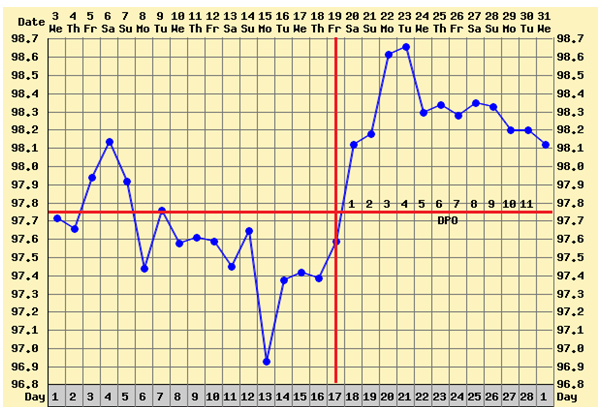
Fig.3. Temperature recording chart
On the other hand, cervical mucous monitoring technique can be used to detect the time of ovulation and possibly the fertile window. The hormonal changes that occur throughout the cycle also have an effect on the amount of mucus secreted by the cervix. Near release of an ovum, the cervix secretes a large amount of mucus unlike when one is about to ovulate when the mucous plug at the cervix is light and thin. This is the time recommended for couples to have sexual intercourse since the chances of conception are highest (Guillebaud, 2012).
Asif M, Jas K, Irwin N & Manit A (2014), ‘Erectile dysfunction,’ Clinical review, 348: 1-9 doi: 10.1136/bmj.g129
Francis, S. H., & Corbin, J. D. (January 01, 2011). PDE5 inhibitors: targeting erectile dysfunction in diabetics, Current Opinion in Pharmacology, 11, 6, 683-8.
Foster, A. M., & Wynn, L. L. (2012). Emergency contraception: The story of a global reproductive health technology. New York, NY: Palgrave Macmillan
Guillebaud, J. (2012). Contraception today: A pocketbook for general practitioners and practice nurses. London: Informa Healthcare.
Glina, S. (April 01, 2011). Erectile Dysfunction after Radical Prostatectomy: Treatment Options. Drugs & Aging, 28, 4, 257-266.
McKerns, Kenneth W. (2012). Reproductive Processes and Contraception. Springer-Verlag.
Perelman, M. A. (January 01, 2011). Erectile dysfunction and depression: screening and treatment, The Urologic Clinics of North America, 38, 2, 125-39.
Runnebaum, B. (2012). Female contraception: Update and trends. Place of publication not identified: Springer.
Thorve, V. S., Kshirsagar, A. D., Vyawahare, N. S., Joshi, V. S., Ingale, K. G., & Mohite, R. J.
(January 01, 2012). Diabetes-induced erectile dysfunction: epidemiology, pathophysiology, and management, Journal of Diabetes and Its Complications, 25, 2.)
MyAssignmenthelp.co.uk is a reputable, genuine and recognized leader in the domain of providing dissertation writing services. We provide students with a unique platform where they can get connected with PhD qualified experts and receive best quality dissertation writing help. Our dissertation writing professionals are committed to helping students write exceptional research-based paper within the deadline provided. Our expertly written dissertations help students acquire their final degree and desired grades.
Upload your Assignment and improve Your Grade
Boost Grades


